Hello
I'm Kaihua Hou
A.K.A. William Hou
Ph.D. Student at UC Berkeley & UCSF
Computational Precision Health (CPH)
About Me CV Publications

Hello
Hello world! I am Kaihua (William) Hou, a Ph.D. student of Computational Precision Health (CPH) at UC Berkeley & UCSF. My research interests lie at the intersection of machine learning (ML), equitable healthcare, and clinical decision-making. The key question directing my research is:
Previously, I was a research assistant working with Emma Pierson and John Guttag at Massachusetts Institute of Technology, where I use probabilistic modeling and machine learning to estimate relative prevalences of underdiagnosed diseases.
At Johns Hopkins University, I built deep learning models for clinical decision-making such as predicting glaucoma worsening, supervised by Jithin Yohannan and Mathias Unberath.
I previously worked on the Delineo COVID modeling project with Anton Dahbura at Johns Hopkins University Information Security Institute. I led various big data research projects using datasets from the Healthcare Cost and Utilization Project (HCUP) under Ali Afshar at Johns Hopkins Medicine.
Let's chat! CV PublicationsDesigning attention architecture for memory-efficient self-supervised learning in medical imaging.
Using large language models and knowledge graph to harmonize and structure clinical text data.
Using probabilistic modeling and machine learning to estimate relative prevalences of underdiagnosed diseases.
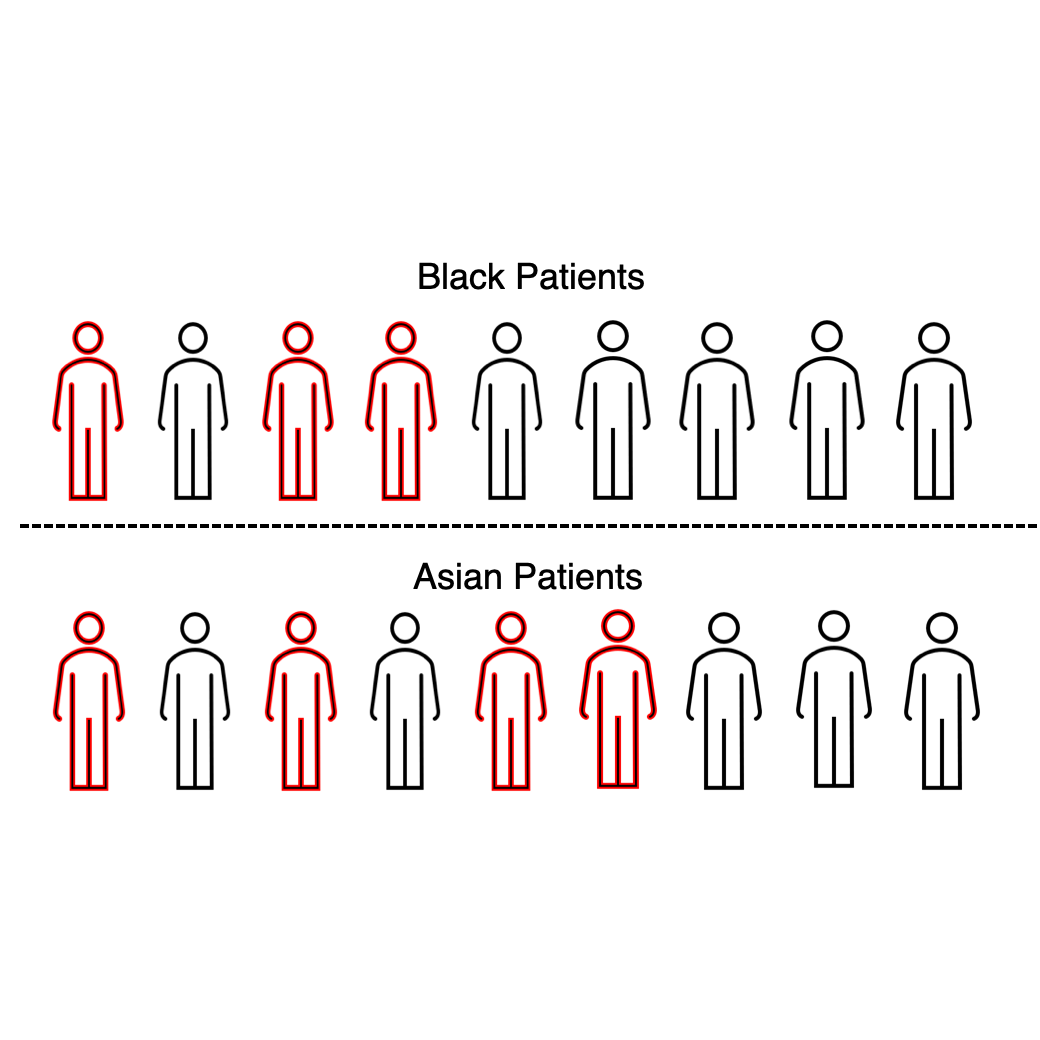
Investigating how different ways of reporting demographic info can affect classic AI for health tasks.
Forecasting rapid glaucoma worsening using LSTM and Transformers.
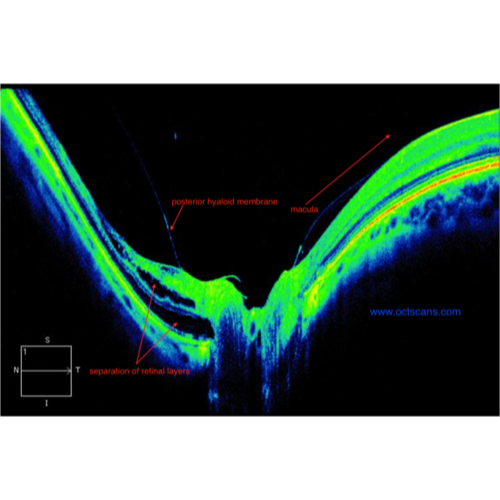
Regenerating visual field measurements with optical coherence tomography data using GAN.
Investigating how AI predictions affect the decision-making process of ophthalmologists.
Analyzing and visualizing six million hospital admissions in the Healthcare Cost and Utilization Project (HCUP).
Developing machine learning models to predict hospital readmission using the HCUP dataset.
Designing and implementing interactive COVID-19 map on county and state level using ReactJS.
Developing statistical disease drivers to model disease spread using population movement information.
Project is publicly launched at Delineo.
Machine Learning
Clinical decision-making
Equitable healthcare
Social behavior & bias
California, U.S.
Ph.D., Computational Precision Health
Maryland, U.S.
B.S., Computer Science
Johns Hopkins University
2022
Johns Hopkins University
2022
California Institute of Technology
2022
The Association for Research in Vision and Ophthalmology (ARVO)
2022
Intuitive Surgical Inc. & Johns Hopkins University
2022
The Association for Research in Vision and Ophthalmology (ARVO)
2022
Whiting School of Engineering, Johns Hopkins University
2022
Johns Hopkins University
Jun. 2020 ~ 2023
Johns Hopkins University
2021 ~ 2023
 view project
view project
Quantifying Disparities in Underreported Health Conditions: An Application to Intimate Partner Violence
npj Women's Health (2024) view project
view project
Coarse race data conceals disparities in clinical risk score performance
ML4H (2023)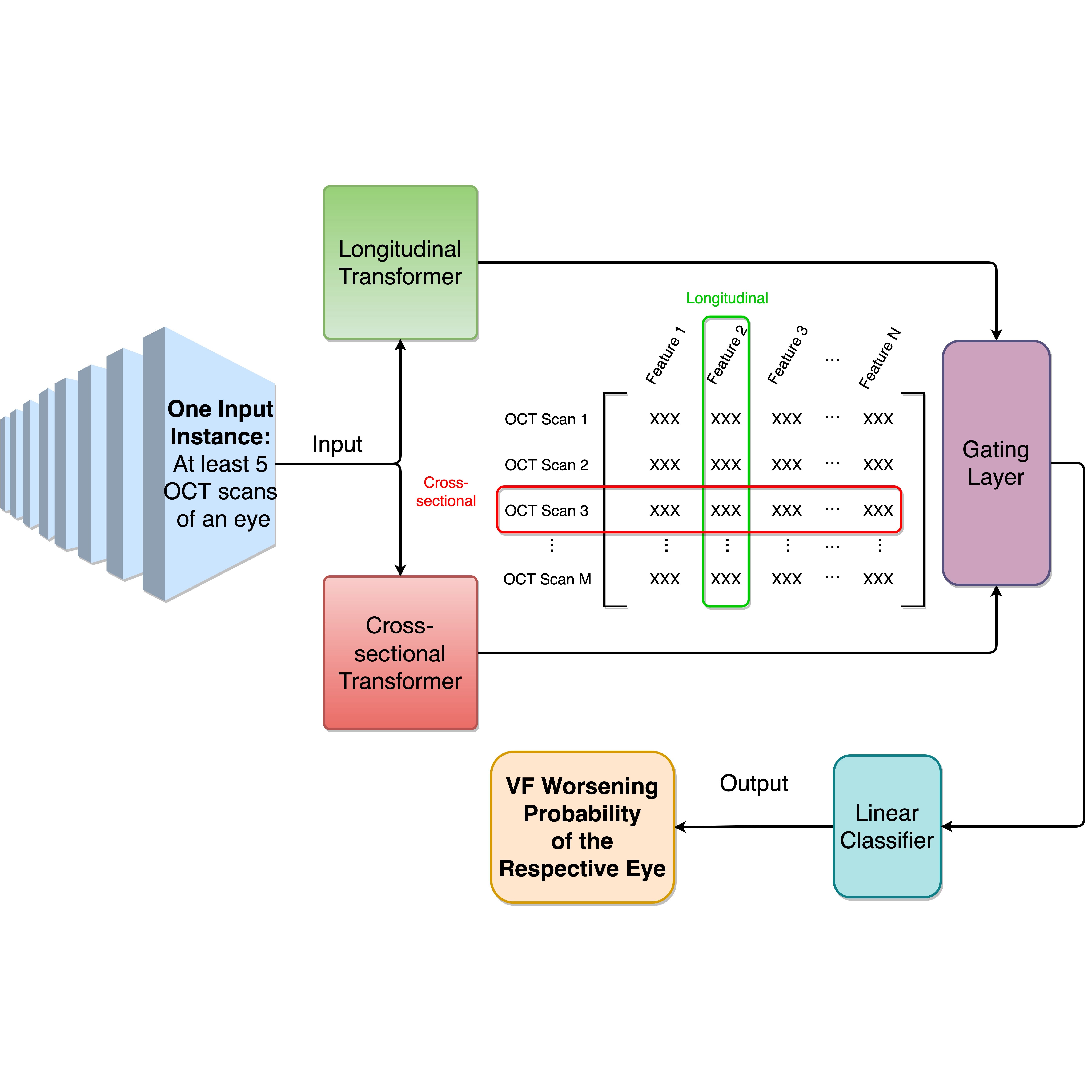 view project
view project
Predicting Visual Field Worsening with Longitudinal Optical Coherence Tomography Data Using a Gated Transformer Network
AAAI (2023)In this project, we aim to predict visual field (VF) worsening from longitudinal optical coherence tomography (OCT) data using a Gated Transformer Network (GTN), and to examine how GTN performance varies for different definitions of visual field worsening and glaucoma severity. A total of 4,211 eyes (2,666 patients) followed at the Johns Hopkins Wilmer Eye Institute with at least five reliable VFs and one reliable OCT within one year of each reliable VF. For each eye, we used three trend-based methods (MD, VFI, and PLR slope) and three event-based methods (GPA, CIGTS, and AGIS) to define VF worsening. Additionally, we created an algorithm, called M6, that classifies an eye as worsening if 4 or more of the 6 aforementioned methods classify the eye as worsening. Using these 7 reference standards for VF worsening, we trained 7 GTNs that accepted inputs of serial OCT scans and output a probability of VF worsening. GTN performance was compared to non-deep learning models from previous studies — linear mixed effects models (MEM) and naïve Bayes classifiers (NBC) — using the same training sets and reference standards as for the GTN. The effect of glaucoma severity on GTN performance was also investigated. The M6 algorithm labeled 63 eyes as worsening. The GTN achieved an AUC (95% CI) of 0.97 (0.88, 1.00) when trained with M6. GTNs trained and optimized with the other 6 reference standards had AUC ranging from 0.78 (MD slope) to 0.89 (AGIS). The 7 GTNs outperformed all 7 MEMs and all 7 NBCs accordingly, though the difference was not statistically significant in one out of the 7 cases (MEM trained with MD slope). GTN performance decreased with increasing glaucoma severity.
 view project
view project
A deep learning model incorporating spatial and temporal information successfully detects visual field worsening using a consensus based approach
Scientific Reports (2023)In this project, we aim at developing a deep learning model using Long Short-Term Memory (LSTM) architecture to predict Visual Field (VF) worsening among a large cohort of glaucoma patients, and comparing its performances with clinician predictions. We trained a 2D Convolutional LSTM to predict VF worsening from the series of VFs for each eye. The reference standard for VF worsening used to train/test the DLM and evaluate clinician performance was defined as a consensus of the automated methods which required at least 4 of the 6 methods to identify worsening. We also sequentially removed VFs that were input into the model to assess the ability of model performance with less data. Our results demonstrated that a DLM trained on a consensus of automated methods successfully identified VF worsening and performed better than clinicians at identifying worsening during routine clinical care, even when using significant less amount of VF data.
 view project
view project
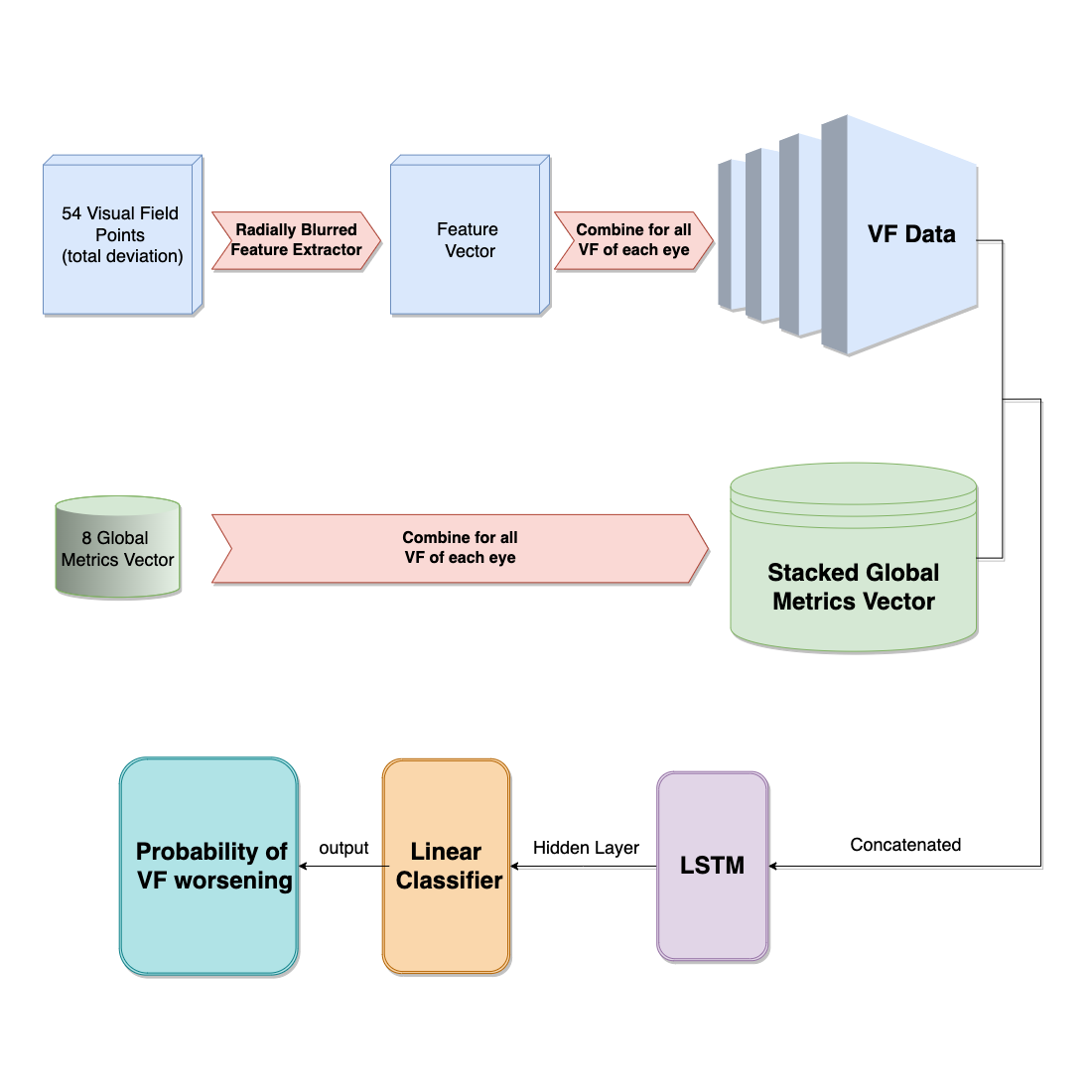
Forecasting Risk of Future Rapid Glaucoma Worsening Using Early Visual Field, Optical Coherence Tomography and Clinical Data
Ophthalmology Glaucoma (2023)We assess whether we can forecast future rapid Visual Field (VF) worsening using deep learning models (DLM) trained on baseline VF, OCT, and clinical data. Additionally, we study the impact of adding additional VF data (beyond baseline) on model performance. The input to the DLM consisted of spatially oriented total deviation values from VF (+/- VF and VF in some models) and spatially oriented RNFL thickness values from the baseline OCT (OCT). We input this VF/OCT stack into a vision transformer feature extractor. We then took the output of the feature extractor and concatenated it with baseline clinical data (Clinical). We then input these combined data through a dense linear classifier to make a final prediction for that eyes’ risk of future rapid VF worsening. We have found that Including baseline data from multiple modalities obtained during routine clinical care (VF, OCT,clinical exam) improves model performance beyond using VF data alone.2 Additionally, adding VF data from subsequent visits further increases model performance. DLMs trained on multimodal data from early visits can forecast future rapid worsening with AUC > 0.8.
 view project
view project
Comparing the Accuracy of Peripapillary OCT Scans and Visual Fields to Detect Glaucoma Worsening
Ophthalmology (2023)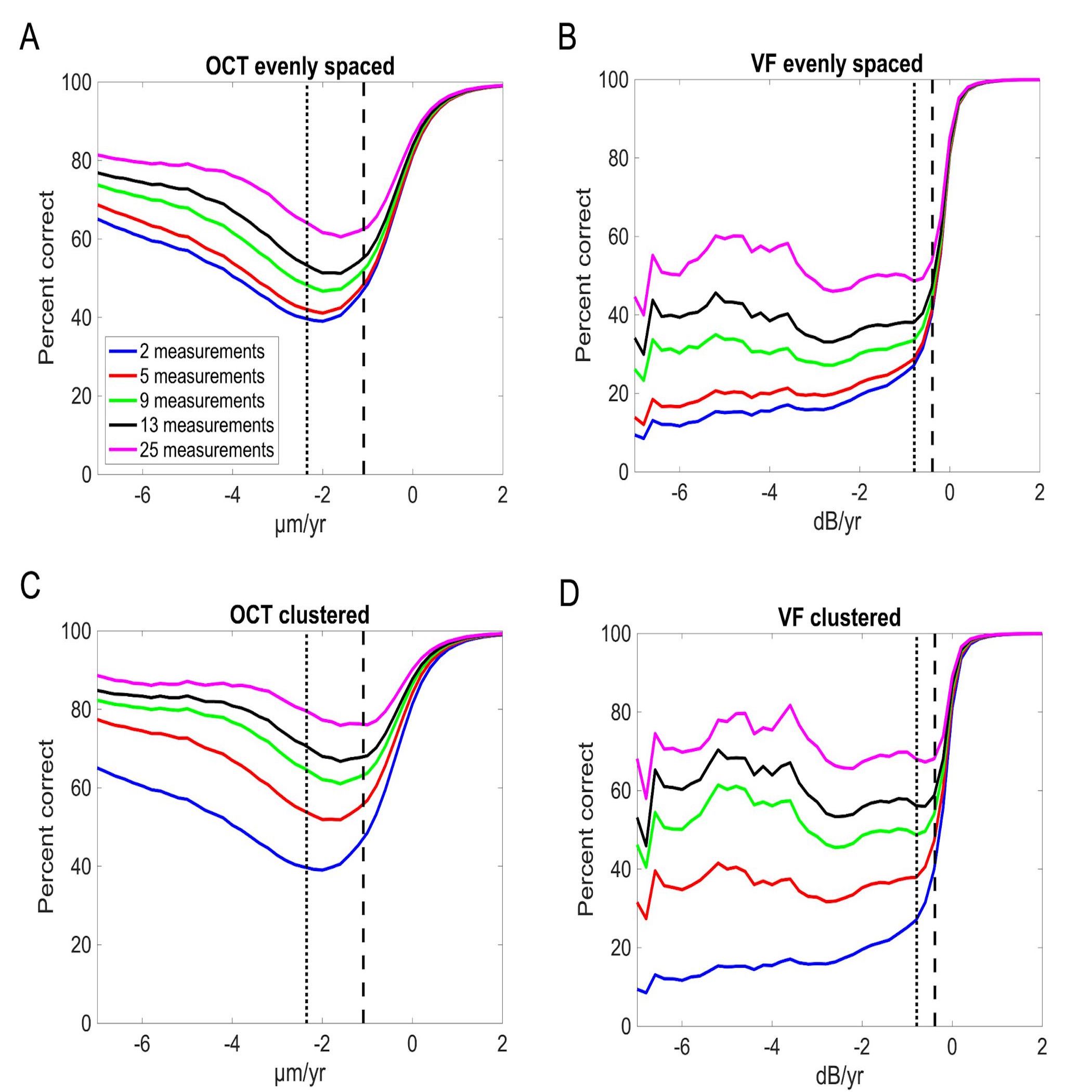 view project
view project
Evidence-Based Guidelines for the Number of Peripapillary OCT Scans Needed to Detect Glaucoma Worsening
Ophthalmology (2023)The aim of this project is to estimate the number of OCT scans necessary to detect moderate and rapid rates of retinal nerve fiber layer (RNFL) thickness worsening at different levels of accuracy using a large sample of glaucoma and glaucoma-suspect eyes. We found that 75th percentile (moderate) and 90th percentile (rapid) rates of RNFL worsening for average RNFL thickness, and the accuracy of diagnosing worsening at these moderate and rapid rates. Thus, in order to more accurately diagnose RNFL worsening, the number of OCT scans must be increased compared to current clinical practice. A clustered measurement strategy reduces the number of scans required compared to evenly spacing measurements.
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua
 Raj Himachal
Raj Himachal
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua
soshiv upreti
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua
gamer king
120 Earl Warren Hall, University of California, Berkeley
2177-2183 University of, Hearst Ave, Berkeley, CA 94709
Category -